765
Views & Citations10
Likes & Shares
Comorbidity or multimorbidity, that is, the presence of two or more
diseases, is a generalized phenomenon that affects the health of populations
throughout the world, with the greatest burden among individuals or
disadvantaged subpopulations, becoming a serious public health problem. Co-infection
is an infection with two or more infectious organisms at the same time.
Co-infections are common in the community, such as coinfection of respiratory
viruses, Influenza A and B, viral and bacterial co-infection with influenza
virus, pulmonary tuberculosis and HIV, HCV and HIV, HBV and HCV, coinfection of
sexual transmission diseases, HIV and parasites, parasitic coinfections and
tropical diseases such as chickungunya and dengue infections, co-infection with
influenza and dengue viruses, malaria and cutaneous leishmaniasis, etc. And all
these multi-infections go through the general medicine practice and frequently
affect patients with other diseases such as hypertension or diabetes mellitus,
COPD, depression, etc. Thus, coinfections must be understood within the broader
concept of comorbidity or multimorbidity. However, many gaps remain in our
understanding of their frequency and importance. Multiple infections can
complicate immunity and treatment, although they can also provide an unexpected
benefit for the patient. In this scenario, this article intends to initiate
some notes for the reflection and systematization of the concepts of
coinfection at the level of general medicine, which is a task that has not yet
begun. For the general practitioner, some important aspects of coinfection are:
the taking of the clinical history and the clues in the recent history of a
patient who can provide evidence of coinfection, the risk factors of
coinfections, the influence of coinfection on the accepted symptoms of each
infection, the frequency of local coinfections, the main and most relevant
coinfections, the impact of coinfection on the course of evolution and
prognosis, the possible effect of drugs in the treatment of coinfections and
the possible problem polypharmacy and its repercussions on the patient,
including adherence to treatment.
Keywords: Coinfection,
Comorbidity, Epidemiology, General practice
INTRODUCTION
It is common situation in general practice that patients say things
like “This cold is lasting twice as much as others” or “I got better from the
flu, but I have relapsed again...” Is it possible to catch two colds at the
same time? Yes; the phenomenon is technically known as coinfection, an
infection with two or more infectious organisms at the same time. Multiple
infections can complicate treatment, although they can also provide an
unexpected benefit to the patient, such as, for example, one organism
suppresses the growth of another.
In nature, organisms are commonly coinfected by two or more strains of
pathogens and have been shown to influence the virulence of the disease.
Co-infections can be especially important for the ecology and evolution of
opportunistic pathogens that are often able to persist and transmit from the
environment. Opportunists, with a wide range of hosts, are more likely to find
potential hosts than pathogens specialized. Since the probability of
coinfections due to opportunistic pathogens transmitted by the environment is
high, the genetic composition of the co-infecting population can lead to
variable results of the infection. In addition, coinfections can select the
most virulent pathogen strains [1].
On the other hand, coinfections modify the immune mechanisms of the
host, but how the systemic and local processes at the site of infection
interact is still unclear [2]. The majorities of studies on coinfections
concentrate on one of the infecting species, an immune function
or group of
The multimorbilidad,
that is to say, the presence of two or more illnesses, is a generalized
phenomenon that affects the health of the populations in the whole world [5].
Generally, when talking about multimorbidity or comorbidity, one tends to think
about the superposition of mental, cardiovascular, diabetes, cancer and
respiratory diseases. But, infectious diseases are not usually included.
However, all the elements that apply to the conceptualization of multimorbidity
or comorbidity can be applied to co-infection. In fact, co-infection should be
understood, from general medicine as comorbidity. There is a broad
international consensus that multimorbidity is best addressed in primary care
settings. These same principles should be applied, as a general rule, to
coinfections.
In this scenario, this
article intends, based on experience and a brief narrative review, to initiate
some notes for the reflection and systematization of the concepts of
co-infection in general medicine level, which is a task that has not yet been
started and it supposes forgetfulness and a dramatic void in the health care
and in the theoretical concepts accepted of morbidity.
DISCUSSION
The family doctor
occupies an important place in the care of the health of the population, its
role as guardian of health implies an action directed mainly to observe and act
on any phenomenon or event that threatens the welfare of the community. The
person is the centre of interest for the family doctor. The three key elements
of general medicine, which are the clinical interview, continuity of care and
attention to context, have fundamental implications in relation to individual
health care and community medicine [6,7].
Family medicine is a
major source of information about health problems and their variation. For most
illnesses the general practitioner is the first point of contact in the health
care system and he looks after a population whose age and sex composition is
known. So, family medicine has important epidemiological connotations,
presenting for example, a unique opportunity to study the natural history of a
disease and to know the rates of diseases in small geographic bases that would
facilitate planning and the adequate use of resources [6,8].
Infectious disease
dynamics offer a wide variety of intriguing and unexplained phenomena. There is
a gap in how diverse studies which encompassing immunology, mathematics,
epidemiology and virology are able to combine to form a complete picture of
this phenomenon. Among these specialties, to study infectious disease dynamics,
family medicine should be included [9].
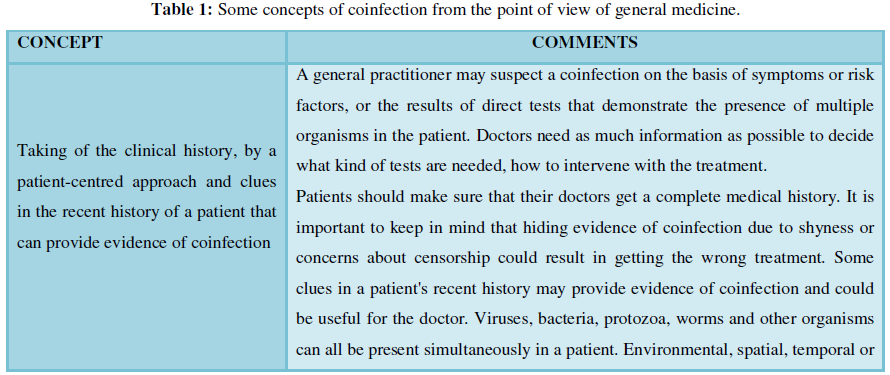
For the general
practitioner, some important aspects about co-infection are: 1) taking of the
clinical history, by a patient-centred approach and clues in the recent history
of a patient that can provide evidence of co-infection; 2) the risk factors of
co-infections; 3) the influence of coinfection on the symptoms accepted of each
infection; 4) frequency of coinfections; 5) the main and the most relevant
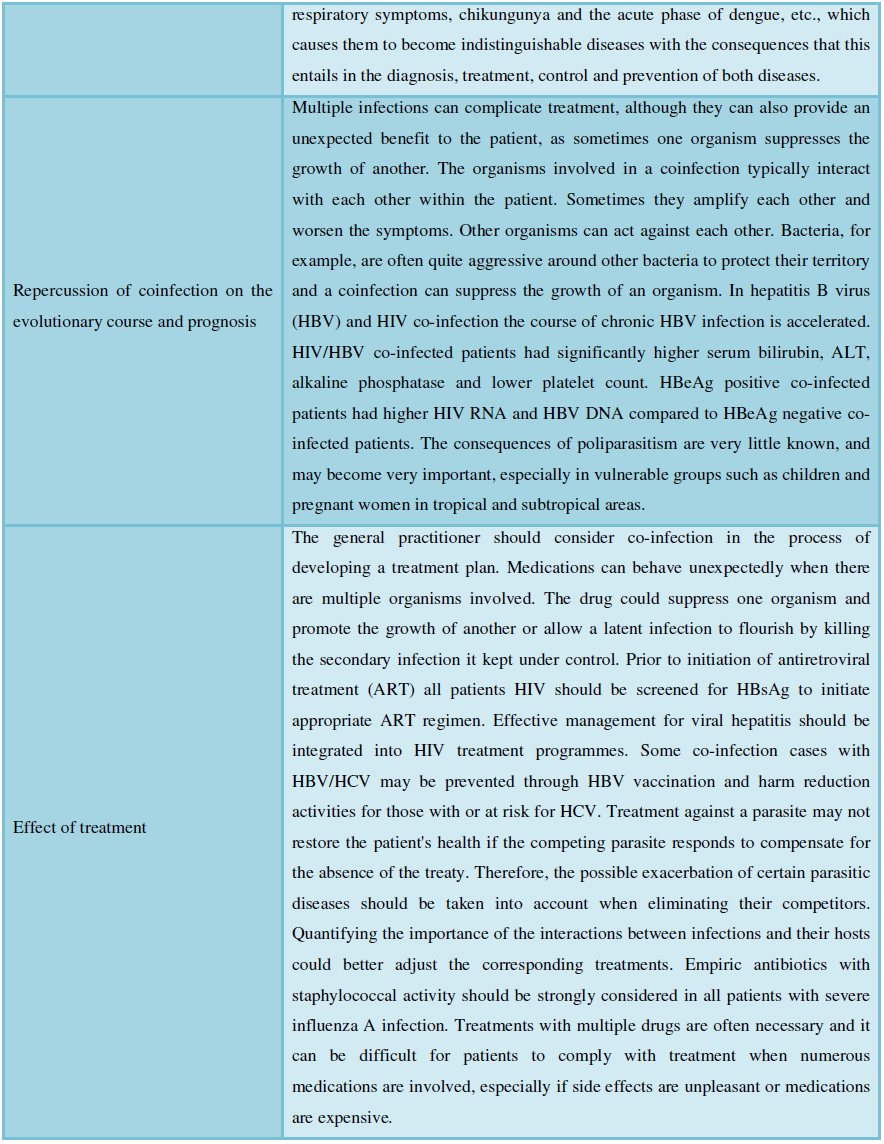
coinfections; 6) the repercussion of coinfection on the evolutionary course and
the prognosis; and 7) the possible effect of the drugs in the treatment of
coinfections and the problematic of the possible polypharmacy and its
repercussions on the patient, including adherence to treatment. Table 1 systematizes and conceptualizes
these elements from the point of view of general medicine/family medicine.
Human immunodeficiency virus, hepatitis C virus, Hepatitis B virus and
tuberculosis
The best data on
coinfection come from studies of these viruses - HIV and HCV. Studies show that
co-infection can worsen, improve or have no impact on the course of a disease.
The result depends on the viruses involved. Progressive immune dysfunction and
the acquired immunodeficiency syndrome (AIDS) develop in most persons with
untreated infection with human immunodeficiency virus type 1 (HIV-1) but in
only approximately 20 to 30% of persons infected with HIV type 2 (HIV-2); among
persons infected with both types, the natural history of disease progression is
poorly understood, but It seems that coinfection with the two main types, HIV-1
and HIV-2, is really beneficial and decreases the progression of the disease.
Results suggest that HIV-1 disease progression is inhibited by concomitant
HIV-2 infection and that dual infection is associated with slower disease
progression. The slower rate of disease progression was most evident in
participants with dual infection in whom HIV-2 infection preceded HIV-1
infection. These findings could have implications for the development of HIV-1
vaccines and therapeutics [10,11].
Clinical studies have
provided compelling evidence that people coinfected with human immunodeficiency
virus (HIV) and Mycobacterium tuberculosis have a 20-30-fold higher risk of
developing active tuberculosis as compared to individuals with M. tuberculosis monoinfection. Studies
have shown that rates of liver disease are higher in persons who are coinfected
with human immunodeficiency virus (HIV) and hepatitis C virus (HCV) than they
are in persons with HCV alone, but estimates of risk vary widely and are based
on data for dissimilar patient populations. There is a significantly elevated
RR of severe liver disease in persons who are coinfected with HIV and HCV. This
has important implications for timely diagnosis and consideration of treatment
in coinfected persons [12].
Hepatitis B virus
(HBV) and HIV co-infection has variable prevalence worldwide. In comparison to
HBV mono-infection, the course of chronic HBV infection is accelerated in
HIV/HBV co-infected patients. HIV/HBV co-infected patients had significantly
higher serum bilirubin, ALT, alkaline phosphatase and lower platelet count.
HBeAg positive co-infected patients had higher HIV RNA and HBV DNA compared to
HBeAg negative co-infected patients. Prior to initiation of antiretroviral
treatment (ART) all patients should be screened for HBsAg to initiate
appropriate ART regimen [13].
HBV/HCV co-infection
identification rates can have declined since the late 1990s, but appropriate
testing and identification for both viruses are important. Some co-infection
cases may be prevented through HBV vaccination and harm reduction activities
for those with or at risk for HCV [14].
Respiratory infections
It can be affirmed
that respiratory infections represent the most important percentage of
infections in family medicine For Fry, in his classic publication, the most
prevalent diseases in general medicine are respiratory infections with 25%
[15]. Co-infection of community-acquired respiratory viruses among patients was
communicated to be of 15%. The most common co-infections were influenza A and
respiratory syncytial virus B and influenza A and enterovirus/rhinovirus [16].
Influenza virus
infection remains a major cause of morbidity and mortality during winter
seasons. Bacterial and virus co-infection is a commonly described situation in
these patients. However, coinfection with influenza A and B, two main types of
influenza virus, seems to occur in less than 2% of cases, but does not appear to
affect the overall outcome. It has been described that Co-infection by
influenza A and B viruses was significantly associated with nosocomial
acquisition. Co-infection was not associated with worse outcome, previous
underlying condition, or vaccination status [17].
Infection by human
rhinovirus (HRV) is a major cause of upper and lower respiratory tract disease
worldwide and displays considerable phenotypic variation. More than 100 viruses
can cause the common cold, so it is not unusual to be exposed to two at the
same time. And, since one virus does not generally confer immunity against the
other, it is not unusual to be infected by two viruses at the same time.
Coinfection in the common cold has been difficult to study in the past due to
the large number of viruses that can cause a cold. In recent years, however,
advances in molecular genetics have allowed scientists to know HRV, the most
common cause of the common cold. All the genetic material of the known strains
of rhinovirus has been sequenced and it has been reported that coinfection with
multiple strains is a common occurrence [18].
It has also been
reported that coinfection provides viruses with the opportunity to mutate into
new strains. Diagnostic tests for many of the viruses that cause common colds
are now commercially available. It has been reported that in children, almost
half of them were infected with more than one virus when they became ill, but
respiratory viral coinfection did not increase severity in all outcomes
assessed. That is, children infected with multiple viruses did not appear to be
sicker than those infected with a single virus, although they stayed sick for
longer [19,20].
With influenza viruses, which cause respiratory
infections similar to those of the common cold, coinfection could be uncommon.
Epidemiological studies, as well as experimental models, suggest that clinical
pictures of viral respiratory infections are often complicated by secondary
bacterial infections. The control of primary viral and secondary bacterial infection
depends on a multifactorial balance between cell,
bacteria and virus, which is seriously disturbed by coinfection. In this review
we analyze the changes in the host cell caused by respiratory viruses and
bacteria that favor coinfection [21]. The coinfection with influenza virus
varies seasonally according to the beginning more or less early of the
influenza season, when other respiratory viruses are less prevalent [22,23].
This co-infection can
occur not only in immunocompromised individuals, but also in immunocompetent
patients. Although co-infection appears to be a rare event, it may still play a
role in the epidemiology, pathogenicity and evolution of influenza viruses
[24]. Co-infection of different influenza A viruses is known to occur but how viruses
interact within co-infection remains unknown. Simultaneous presence of the two
influenza viruses increases the infectivity and the transmissibility of A/H1N1
virus but whether it changes the infectivity of A/H3N2 is unclear. In
conclusion is suggested that influenza A viruses within co-infected patients
can interact in some ways rather than transmit independently and this can
enhance the spread of influenza A virus infection [25].
Bacterial
co-infections in severe influenza infection were common, resulted in delay of
antiviral therapy and were associated with increased resource allocation and
higher mortality [26]. Bacterial co-infection was frequent in influenza A H1N1
pneumonia, with COPD and increased platelet count as the main predictors.
Although associated with higher severe scales at admission, bacterial
co-infection did not influence mortality of these patients [27].
Chickungunya and dengue infections and co-infection of the mosquito Aedes aegypti
Dengue-chikungunya
coinfections can occur if the person is bitten by two mosquitoes infected with
the different viruses or if a mosquito is infected by both viruses. Since there
is neither a vaccine nor a specific treatment, the treatment focuses on the
control of the symptoms, but despite this, the non-differentiation of both
diseases can cause serious consequences. During outbreaks of dengue, or in
countries that historically suffer from dengue epidemics, doctors tend not to
confirm their diagnosis in the laboratory and it is usually assumed that it is
a dengue infection. The Aedes aegypti
mosquito spreads both dengue and chikungunya and is endemic in 174 countries
and the Aedes albopictus mosquito,
which also spreads both viruses, is adaptable to less extreme climates. The
vector species that spread these pathogens and also the Zika virus - are the
same; however, the number of countries that have reported cases of dengue is
considerably higher than the countries that have reported Chikungunya, which
can be caused for the widespread misdiagnosis of chikungunya with dengue
[28,29].
Co-infection of the
mosquito Aedes aegypti with two
microsporidian parasites (Vavraia culicis
and Edhazardia aedis) at two
levels of larval food availability affects parasite transmission directly and
indirectly through effects on host traits. Co-infections may modify parasite
transmission opportunities directly as a consequence of interactions in the
within-host environment, but also indirectly through changes in host life
history. Furthermore, host and parasite traits are sensitive to the abiotic
environment with variable consequences for parasite transmission in
co-infections. Co-infection can negatively affect parasite transmission
opportunities, both directly as well as indirectly via effects on host life
history [30].
Sexually transmitted infections
Co-infection between
different sexually transmitted infections (STIs) is very frequent. Therefore,
anyone who presents one of them should rule out the presence of others,
particularly HIV infection and chlamydia infection [31].
Parasitic co-infections
They are common in
nature and the interactions between different species of parasites are similar.
So far, very few studies have been carried out on the interactions that occur
during these coinfections, despite their undoubted influence on the dynamics of
parasitic diseases and their consequences.
It is assumed that the
different species of parasites that colonize a given host usually do not
interact because they often parasitize different tissues and the use of
different resources limits competition. In mixed infections, treatment against
a parasite may not restore the patient's health if the competing parasite
responds to compensate for the absence of the treaty. Therefore, the possible
exacerbation of certain parasitic diseases should be taken into account when
eliminating their competitors [32].
Individuals living in
areas endemic for helminths are commonly infected with multiple species.
Variability in risk of N. americanus
and S. mansoni co-infection between
households cannot be entirely explained by exposure-related risk factors,
emphasizing the possible role of other household factors in the heterogeneous
distribution of helminth co-infection. Untangling the relative contribution of
intrinsic host factors from household and environmental determinants therefore
remains critical to our understanding of helminth epidemiology [33].
CONCLUSION
1. Kinnula H, Mappes J, Sundberg LR (2017)
Coinfection outcome in an opportunistic pathogen depends on the inter-strain
interactions. BMC Evol Biol 17: 77.
2. Nikita HT, Jieh-Juen Y, Chiung-Yu H, Doelger
RP, Navara CS, et al. (2018) Microbial co-infection alters macrophage
polarization, phagosomal escape and microbial killing. Innate Immun 24:
152-162.
3. Thakar J, Pathak AK, Murphy L, Albert R,
Cattadori IM (2012) Network model of immune responses reveals key effectors to
single and co-infection dynamics by a respiratory bacterium and a
gastrointestinal helminth. PLoS Comput Biol 8: e1002345.
4. Griffiths EC, Pedersen AB, Fenton A, Petchey
OL (2015) Reported co-infection deaths are more common in early adulthood and
among similar infections. BMC Infect Dis 15: 411.
5. Turabian JL, Perez FB (2016) A way of helping
“Mr. Minotaur” and “Ms. Ariadne” to exit from the multiple morbidity labyrinth:
The “master problems”. Semergen 42: 38-48.
6. Turabian JL (2018) Community medicine from
the point of view of the general practitioner: Never plump your foot straight
into your shoe in the morning. Int J Adv Comm Med 1: 44-50.
7. Turabian JL (2017) A narrative review of
natural history of diseases and continuity of care in family medicine. Arch
Community Med Public Health 3: 041-047.
8. Turabian JL, Moreno-Ruiz S, Cucho-Jove R
(2016) Epidemiology in family medicine. J Gen Pract (Los Angel) 4: 278.
9. Turabian JL (2017) The variation of seasonal
diseases in family medicine depends on infectious diseases and these are mainly
respiratory diseases. J Gen Pract (Los Angel) 5: 309.
10. Esbjörnsson J, Månsson F, Kvist A, Isberg PE,
Nowroozalizadeh S, et al. (2012) Inhibition of HIV-1 disease progression by
contemporaneous HIV-2 infection. N Engl J Med 367: 224-232.
11. González-García JJ, Mahillo B, Hernández S,
Pacheco R, Diz S, et al. (2005) Prevalences of hepatitis virus coinfection and
indications for chronic hepatitis C virus treatment and liver transplantation
in Spanish HIV-infected patients. The GESIDA 29/02 and FIPSE 12185/01
Multicenter Study. Enferm Infecc Microbiol Clin 23: 340-348.
12. Graham CS, Baden LR, Yu E, Mrus JM, Carnie J,
et al. (2001) Influence of human immunodeficiency virus infection on the course
of hepatitis c virus infection: A meta-analysis. Clin Infect Dis 33: 562-569.
13. Sarkar J, Saha D, Bandyopadhyay B, Saha B,
Kedia D, et al. (2016) Baseline characteristics of HIV and hepatitis B virus
(HIV/HBV) co-infected patients from Kolkata, India. Indian J Med Res 143:
636-642.
14. Fang L, Yu A, Buxton JA (2009) Identification
of chronic hepatitis B and hepatitis C co-infection in British Columbia from
1991 to 2007. Can J Public Health 100: 349-352.
15. Fry J (1987) Common diseases. Their nature,
incidence and care. MTP Press Limited, Lancaster, England.
16. Peci A, Winter A, Gubbay JB, Skowronski DM,
Balogun EI, et al. (2013) Community-acquired respiratory viruses and co-infection
among patients of Ontario sentinel practices, April 2009 to February 2010.
Influenza Other Respir Viruses 7: 559-766.
17. Pérez-García F, Vásquez V, de Egea V, Catalán
P, Rodríguez-Sánchez B, et al. (2016) Influenza A and B co-infection: A case-control
study and review of the literature. Eur J Clin Microbiol Infect Dis 35:
941-946.
18. Palmenberg AC, Spiro D, Kuzmickas R, Wang S,
Djikeng A, et al. (2009) Sequencing and analyses of all known human rhinovirus
genomes reveal structure and evolution. Science 324: 55-59.
19. Martin ET, Fairchok MP, Stednick ZJ, Kuypers
J, Englund JA (2013) Epidemiology of multiple respiratory viruses in childcare
attendees. J Infect Dis 207: 982-989.
20. Comerlato SM, Coutinho BV, Chakr G, de Moura
A, Garces BR, et al. (2016) Respiratory viral coinfection and disease severity
in children: A systematic review and meta-analysis. J Clin Virol 80: 45-56.
21. Arrevillaga BG, Gómez García B (2006)
Aspectos moleculares de coinfecciones de virus respiratorios con bacterias. Enf
Inf Microbiol 26: 115-122.
22. Reynders M, De Foor M, Hombrouck A, Epalza C,
Dediste A, et al. (2018) Viral co-infections involving influenza A: Changes
observed during the 2009 pandemic season. Infect Dis Diagn Treat.
23. Turabian JL, Cucho-Jove R, Moreno-Ruiz S
(2017) Conceptual implications of family medicine in the study of the seasonal
variation of diseases: A narrative review. CP Epidemiol 1: 001.
24. Pando R, Drori Y, Friedman N,
Glatman-Freedman A, Sefty H, Shohat T, et al. (2017) Influenza A (H1N1) pdm
2009 and influenza B virus co-infection in hospitalized and non-hospitalized
patients during the 2015-2016 epidemic season in Israel. J Clin Virol 88: 12-16.
25. Zhang XS, De Angelis D (2016) Construction of
the influenza A virus transmission tree in a college-based population:
Co-transmission and interactions between influenza A viruses. Infect Dis 16:
38.
26. Shah NS, Greenberg JA, McNulty MC, Gregg KS,
Riddell J, et al. (2016) Bacterial and viral co-infections complicating severe
influenza: Incidence and impact among 507 U.S. patients, 2013-2014. J Clin
Virol 80: 12-19.
27. Cillóniz C, Ewig S, Menéndez R, Ferrer M,
Polverino E, et al. (2012) Bacterial co-infection with H1N1 infection in
patients admitted with community acquired pneumonia. J Infect 65: 223-230.
28. Furuya-Kanamori L, Liang S, Milinovich G,
Ricardo J. Soares M, et al. (2016) Co-distribution and co-infection of
chikungunya and dengue viruses. BMC Infect Dis.
29. Turabián JL, Moreno-Ruiz S, Cucho-Jove R
(2016) “Doctor, I have Chikungunya”. Conceptual systematisation of specific
epidemiological implications in family medicine. Semergen 42: 488-491.
30. Duncan AB, Agnew P, Noel V, Michalakis Y
(2015) The consequences of co-infections for parasite transmission in the
mosquito Aedes aegypti. J Anim Ecol
84: 498-508.
31. Díez M, Díaz A (2011) Sexually transmitted
infections: Epidemiology and control. Rev Esp Sanid Penit.
32. Manzano-Román R, Oleaga A, Pérez-Sánchez R,
siles-Lucas M (2012) Coinfecciones parasitarias: Influencia de las
interacciones. Organización Colegial Veterinaria Española.
33. Pullan RL, Bethony JM, Geiger SM, Cundill B,
Correa-Oliveira R, et al. (2008) Human helminth co-infection: Analysis of
spatial patterns and risk factors in a Brazilian community. PLoS Negl Trop Dis
2: e352.
-
 Table 1
Table 1 -
Table 2
-
Table 3

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Pathology and Toxicology Research
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)


